What hormones do my adrenal glands produce?
The adrenal cortex produces three hormones, from three different layers:
1. Mineralocorticoids: the most important of which is aldosterone. This hormone helps to maintain the body’s salt and water balance, which is important for maintaining blood pressure. Aldosterone helps the kidney conserve salt when it is needed. It acts in the kidney to cause sodium and water to be retained, and potassium to be lost. This action is important if the body has low salt and water levels, that could risk a low blood pressure. However, too much aldosterone can cause high blood pressure (hypertension) and low potassium. Without aldosterone (for example if the adrenal glands are not working properly), the kidney loses excessive amounts of salt (sodium) and, consequently, water, leading to severe dehydration and low blood pressure. In summary, if we do not have enough salt in the body, aldosterone production is ‘switched on’ and the kidney retains salt, but if we have too much salt, the amount of aldosterone being made is reduced and the kidney can excrete the excess salt.
In nonepithelial target cells, mineralocorticoid signaling has been linked to various physiological processes, such as memorization and learning, stress response, neuroprotection and regulation of sodium appetite (hippocampus)
Mineralocorticoids
- Mineralocorticoids are hormones secreted by the adrenal cortex.
- Aldosterone is the primary mineralocorticoid secreted by the gland.
- The main functions of this hormone include:
- Maintaining the salt-water balance in the body by acting on two important minerals (electrolytes) namely sodium and potassium.
- It enhances sodium reabsorption and potassium excretion from the kidneys.
- It also reduces sodium loss from the body by increasing the reabsorption of sodium from sweat, saliva, and bile.
- It also reduces water loss from the body's reabsorption of water from urine.
2. Glucocorticoids: predominantly cortisol, which is also known as the body’s ‘natural steroid’. This hormone is involved in the response to illness and also helps to regulate body metabolism. Cortisol is released during the ‘stress response’ to illness. Cortisol stimulates glucose production to help maintain blood glucose levels. Cortisol also has anti-inflammatory effects especially at higher amounts.
3. Adrenal androgens: these male sex hormones, mainly dehydroepiandrosterone (DHEA) and testosterone, are present in both men and women. All have weak effects, but play a role in early development of the male sex organs in childhood, and are important for the normal onset of female body hair following puberty.
Adrenocorticotropic hormone (ACTH), secreted by the anterior pituitary gland, primarily affects the release of glucocorticoids and adrenal androgens by the adrenal gland and, to a much lesser extent, also stimulates aldosterone release.
The adrenal medulla produces catecholamines:
Catecholamines include adrenaline, noradrenaline and small amounts of dopamine – these hormones are responsible for all the physiological characteristics of the stress response, the so called 'fight or flight' response, which can include increased heart rate, blood pressure, breathing rate, dilated pupils in the eye, and looking flushed or pale.
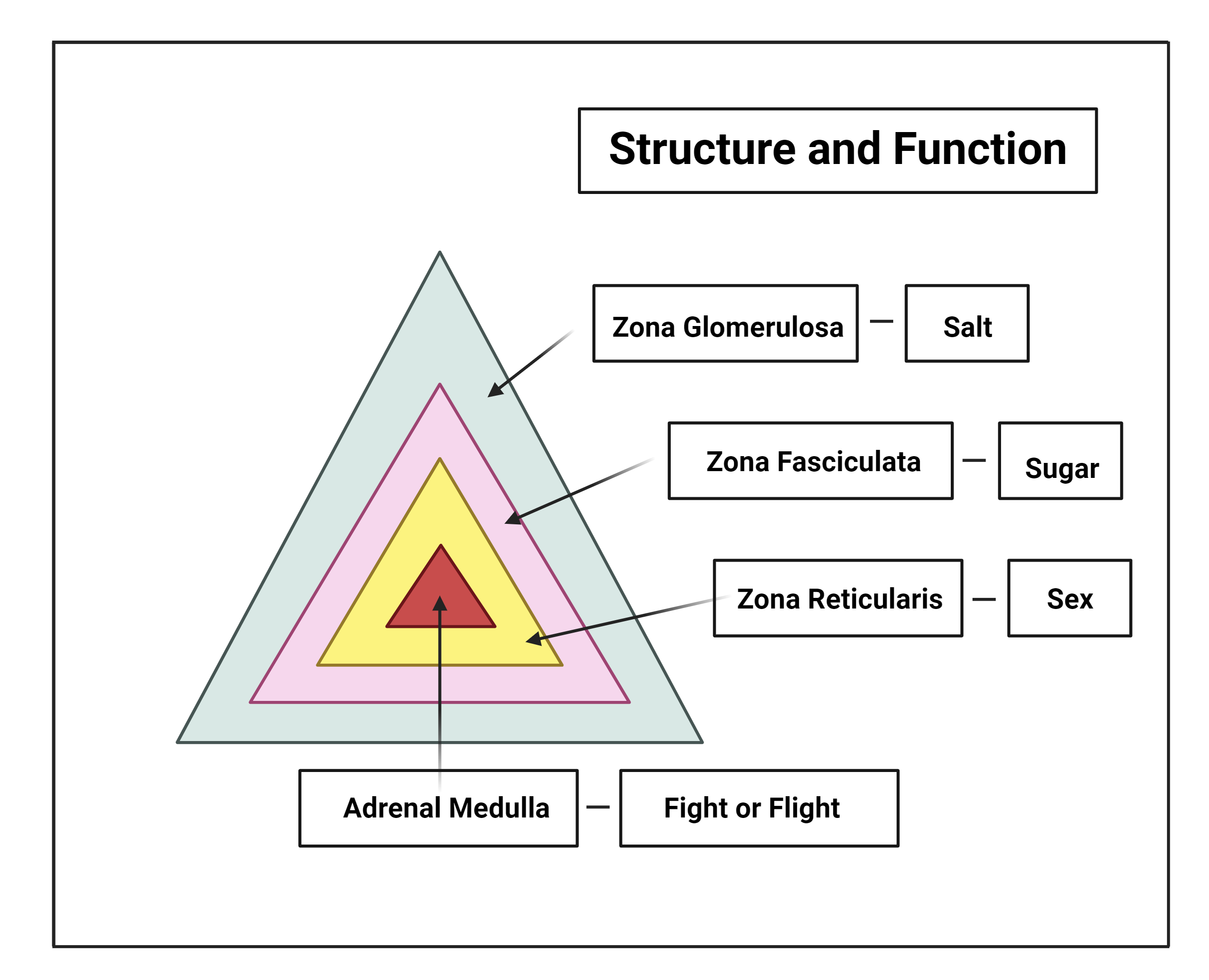
Diagrammatic representation of adrenal gland structure and function. Created with BioRender.com
What could go wrong with my adrenal glands?
Overproduction of aldosterone can occur, sometimes due to a benign tumour of the adrenal gland, which causes a condition known as primary hyperaldosteronism (or Conn’s Syndrome). Aldosterone causes sodium and water retention in the kidneys and loss of potassium in the urine. Excess aldosterone causes high blood pressure (hypertension), which can be resistant to conventional blood pressure control tablets, and can be associated with low potassium in the blood (hypokalaemia). Some studies have suggested that hyperaldosteronism may account for up to 5% of all people with high blood pressure and an even higher proportion (up to 20%) of those who have difficult to control hypertension.
In rare cases, the adrenal glands can become either overactive or underactive. The two main glucocorticoid-related disorders resulting from these are Cushing's syndrome (overactive) and Addison's disease (underactive).
Cushing's syndrome is due to overactive adrenal glands from excessive production of cortisol. This can either be due to a benign tumour in the adrenal gland over producing cortisol, or due to excess ACTH from a tumour in the pituitary gland or elsewhere. Signs and symptoms can include thinning or easy bruising of the skin, purple or red stretch marks (‘striae’), truncal obesity, diabetes, psychiatric disturbances, high blood pressure, muscle weakness (especially the large proximal muscles like the thighs), osteoporosis, excessive facial hair and irregular periods in women. It can also result in growth failure in children. Patients with cortisol excess can also have impaired wound healing and an increased susceptibility to infection. People with Cushing’s syndrome may have characteristic rounding of the face and redness of the cheeks.
Addison's disease or primary adrenal insufficiency, is due to underactive adrenal glands associated with lack of hormones usually produced by the adrenal cortex ie cortisol, aldosterone, and androgens. Adrenal insufficiency may be acute or chronic. Symptoms of chronic adrenal insufficiency include low blood pressure, fatigue, weight loss, anorexia, nausea, vomiting, abdominal pain, salt craving and low blood sugar. Skin, especially the skin creases, and mucous membranes such as around the gums, may show increased pigmentation. The loss of secondary sex characteristics is more likely to occur in women with the disease, as men are less reliant on adrenal androgens given that they can also produce sufficient testosterone from the testes.
Acute adrenal insufficiency is a medical emergency and must be identified and promptly treated. The hallmarks of acute adrenal insufficiency are circulatory collapse with abdominal pain and low blood sugar. In the emergency situation hydrocortisone is given by injection, either into the vein or into the muscle. Thereafter, cortisol is replaced with daily hydrocortisone or prednisolone tablets and aldosterone is replaced with fludrocortisone tablets. It is important to know that during illness it is necessary to increase the intake of hydrocortisone tablets to replicate the increased steroid production that the body would usually make in times of illness (but is unable to do so due to failure of the adrenal glands).
Sometimes secondary adrenal insufficiency might occur if a patient has been on steroid treatment for a long period of time, for example, to treat asthma, or other chronic inflammatory diseases. These steroids, especially if given at high doses for a prolonged duration, can cause negative feedback on the hypothalamus / pituitary to reduce the production of ACTH This reduction in ACTH can, in turn, lead to reduced production of steroids by the adrenal glands, which can in time wither due to lack of stimulation. If the steroid medication is stopped abruptly, this can leave patient deficient of any steroids as the adrenal glands can no longer make enough steroids. This can be a dangerous situation as steroids are necessary for health. Therefore, gradually ‘weaning’ down doses of steroid medications, especially if they have been used for a prolonged period is advisable, under medical supervision, to ensure that the adrenal glands are able to work properly again, and produce the required amount of steroids for health before the steroid medication is stopped.
Overproduction of androgens is rare but may result in excessive hair growth and menstrual period disturbances. Tumours of the adrenal gland are mostly benign, but sometimes result in over- or under-production of adrenal hormones. Adrenal cancer is very rare. Adrenal tumours may require surgery if they are large or overproduce hormones.
Phaeochromocytoma is a tumour of the adrenal medulla, and can release excess amounts of catecholamines. This can lead to high blood pressure, headaches, sweating, tremors and fast heart rate. Most of these tumours are discovered incidentally when people undergo scans for other reasons, although some may be linked with conditions that run in families such as Von Hippel Lindau disease.
The treatment of each disorder varies according to the specific cause. Patients with any concerns about these conditions should seek advice from their doctor or an experienced healthcare professional.
Post a Comment